
Hearing loss comes in many shapes and sizes. With all the variations in hearing loss, it is important to understand the different types of solutions available. One solution may be more appropriate than another given the type, severity and etiology (cause) of the hearing loss. Conventional hearing aids are appropriate for mild to severe hearing loss, but a hearing implant may be better for a severe to profound hearing loss. Patients with unilateral hearing loss – like Single-Sided Deafness (SSD), with one normal functioning ear and one deaf ear – are now being considered potential implant candidates for either a Bone Anchored Hearing System (BAHS) or a Cochlear Implant (CI).
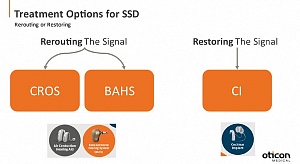
With SSD, most people are familiar with a CROS or BiCROS system. These devices work by transmitting sound wirelessly from the deaf ear into the better ear. CROS/BiCROS is often the first treatment option considered because clinicians are most familiar with this solution, and it does not require surgery. However, for patients who are unsuccessful with a CROS/BiCROS, it may be time to discuss an implant!
Bone Anchored Hearing Systems (BAHS) for SSD
A BAHS is a hearing device that transmits sound through vibrations of the skull. Rather than sending an acoustic signal through the ear canal to the inner ear (air conduction pathway), the signal is transformed into vibrations and sent via the skull to the inner ear (bone conduction pathway). Bone conduction is the reason why you think ‘do I really sound like that?!’ when you hear yourself on a recording. When you listen to a recording of your own voice, you are missing the sound transmitted via bone conduction.
Patients with SSD can take advantage of this bone conduction pathway by using a BAHS to transmit sound from their deaf side to their better ear via vibration of the skull. The BAHS is placed on the deaf ear where it picks up sound, converts the sound into vibrations which are then sent along the skull to the opposite (good) ear. One of the major benefits of this type of system compared to a CROS is that both ears
remain completely open – there is nothing sitting in the ears. Another advantage is that you only need to wear ONE device. Nothing is required on the good ear.
A BAHS can be worn surgically (recommended) on an abutment or non-surgically on a headband. The benefit of implantation is better access to sound, improved aesthetics, and comfort. With a surgically worn BAHS, there is no skin in the way dampening the sound, meaning users get an extra boost in the pitches responsible for speech clarity and understanding. Additionally, when implanted, there is no need for a headband, making it a more discreet option with no sensation of pressure:
 |
 |
BAHS vs. CROS for SSD
Remember that these are two different systems that function in a similar way – by rerouting the signal from the deaf ear to the good ear. There are pros and cons to choosing one system over the other and it usually comes down to patient preference and subjective benefit from a trial with each system. Benefits to choosing a BAHS for SSD from the literature:
-
Patient’s subjective benefit rated higher than with CROS
-
Better speech understanding in noise compared to CROS System
-
Subjective tinnitus ratings decreased over 6 and 12m of BAHS usage
-
Higher rates of retention compared to CROS
Cochlear Implants (CI) for SSD
.png)
A cochlear implant is a hearing device that converts sound in your environment into an electrical signal that is sent via your hearing nerve to be interpreted by your brain. It is a device for individuals who have a severe to profound sensorineural hearing loss, and for whom conventional hearing aids are not sufficient.
A cochlear implant is another implantable solution for SSD. This type of implant is different from a BAHS in that with a CI, we are attempting to restore the hearing in the poor/deaf ear. One major advantage of this treatment option compared to CROS or BAHS, is that patients will have access to sound through both ears. It is well documented that hearing with two ears is beneficial. These benefits include better speech understanding in noise and improved localization.
There are several other advantages to cochlear implantation for SSD:
-
Improvements in:
-
speech-in-noise perception for adults
-
isolated speech perception using only the implanted ear
-
speech understanding in background noise in children
-
-
Long-term improvements in localization and subjective improvements in speech intelligibility and spatial hearing
- Potential improvement in tinnitus symptoms 1-2 months post-activation
Candidacy for a CI is more complex than with a CROS or a BAHS. Given the complexity of the surgery and the different method of hearing that is achieved with a CI (hearing by electrical stimulation rather than acoustic), there are more factors that need to be considered in determining candidacy for CI:
-
Duration of deafness
-
Cause of deafness
-
Age of patient (In Canada there is no upper age limit for a CI)
-
Medical comorbidities/general health of patient
-
Patient’s motivation and dedication to better hearing
How do I know if a BAHS, CROS or CI is best for me?
To start, identify what your main goals are with amplification; is it to hear better in noise? Regain hearing in your deaf ear? Improve your sound awareness? Answering these questions will be helpful in determining which solution(s) is most appropriate. This table summarizes the benefits/ considerations for each system:
| CROS/BiCROS | BAHS | CI |
|---|---|---|
|
|
|
Questions to ask your Audiologist
-
Am I a candidate for a BAHS or CI?
-
Is there funding for BAHS or CI in my province?
-
Where can I get a BAHS or CI?
-
Are there patients I can speak with who have been through this process before?
To learn more about BAHS and CI, visit https://www.oticonmedical.com/ca.

Jenny Harris, M.Cl.Sc., Reg. CASLPO, is an audiologist with Oticon Medical Canada, a bone anchored hearing system and cochlear implant manufacturer. She is the Clinical Support and Business Development Manager for BAHS and CI. Based on her clinical background, Jenny is passionate about sharing her knowledge on implant candidacy and technology. Prior to joining Oticon Medical , Jenny worked for the Infant Hearing Program in Ontario.